
The Low-Dose Illusion: When 0.25 mg Means Two Different Things
Picture two people, needle in hand, both drawing up 0.25 mg of semaglutide once a week. One is a patient in week two of a doctor’s standard titration schedule. The other has been holding at that same number for months, by choice, without a prescriber’s say-so. Chemically, the syringes are identical. Biologically, the receptor on the other end doesn’t care who ordered the dose or why. And yet these are not the same practice, and the difference between them explains most of what goes right, and wrong, in the world of GLP-1 microdosing.
What the molecule is actually doing
Semaglutide and tirzepatide work by mimicking a gut hormone called GLP-1, glucagon-like peptide-1, which your intestine releases after a meal. The hormone nudges the pancreas to release insulin, slows down how fast the stomach empties, and sends a fullness signal to the brain. Tirzepatide adds a second signal, mimicking a related hormone called GIP. Neither drug is smart. The receptor responds to how much drug is present and for how long, full stop. It has no way of knowing whether a clinician wrote the prescription or a forum thread suggested the number.
That’s the mechanistic reason every approved regimen starts low and works upward. Semaglutide’s labeled path begins at 0.25 mg weekly and steps up toward a 2.4 mg maintenance dose for weight management; tirzepatide starts at 2.5 mg and climbs from there. Starting low isn’t about caution for its own sake, it’s about giving the gut time to adjust, since nausea, vomiting, diarrhea, and constipation cluster hardest during the early climb.
So if the pharmacology alone can’t distinguish supervised titration from microdosing, what does? Four things, and none of them are chemical.
The trials tell you where the destination is, not where you can stop
Here’s where the trial data becomes essential, and also where it gets easy to mislead yourself. In STEP 1, adults taking weekly semaglutide up to 2.4 mg lost an average of 14.9% of body weight over 68 weeks, against 2.4% on placebo, in a study of nearly 2,000 people [2]. In SURMOUNT-1, tirzepatide produced average reductions of 15.0%, 19.5%, and 20.9% at the 5 mg, 10 mg, and 15 mg doses over 72 weeks [3]. Those are big, well-earned numbers, and they describe one specific thing: what happens when someone reaches a target dose and stays there.
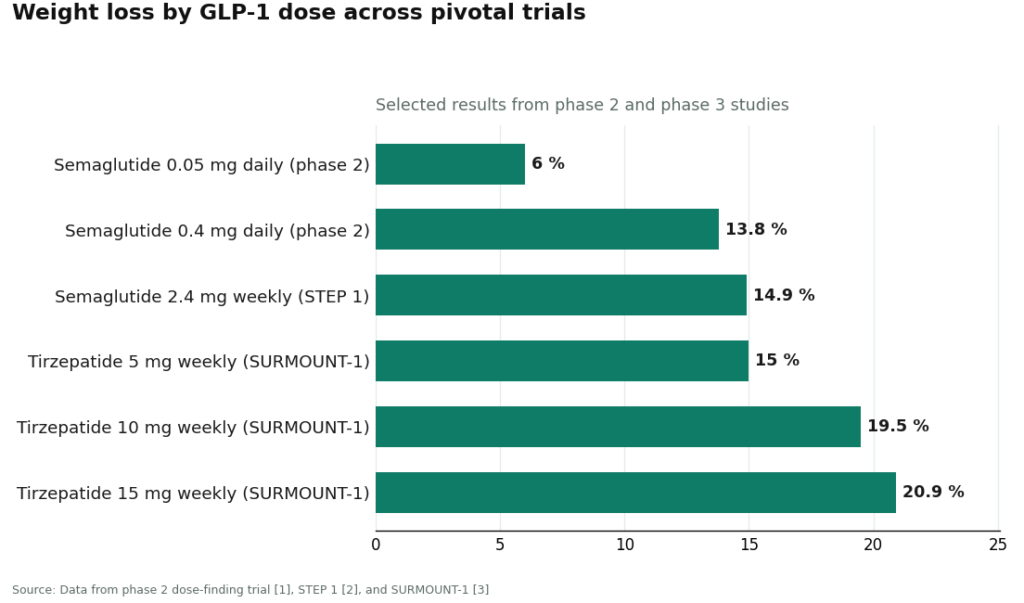
There’s also older, quieter data worth pulling forward. A phase 2 dose-finding trial tested daily semaglutide from 0.05 mg up to 0.4 mg in adults with obesity and found a clean, orderly relationship between dose and weight loss. Even the lowest dose tested, 0.05 mg daily, produced roughly 6% average weight loss at one year, compared with about 2.3% on placebo, and the top dose reached about 13.8% [1]. That trial proves something real: a low dose is not biologically inert. It does something.
What it doesn’t prove is the thing microdosing implicitly claims, that holding low is a durable strategy worth adopting on purpose. The dose-finding study was built to identify a target for further development, using daily injections rather than the weekly schedule most people actually use. Nobody tested what happens if you deliberately stop climbing and just stay at the bottom for months or years. That’s the gap. The trials map the road to the destination. Nobody has mapped what happens if you get off early and camp there.
See also: Understanding Myers’ Cocktail IV Therapy: The Classic Vitamin Infusion
Four places where the same dose stops being the same thing
Who decided. In standard titration, a licensed clinician weighed the patient’s history, checked for contraindications, and chose the pace. If someone can’t tolerate escalation, a clinician holding them at a lower dose is an ordinary clinical judgment call about one specific person. In the gray-market version, the decision-maker is a checkout page, a podcast, or the patient’s own reading of a forum thread. Same number, entirely different process behind it.
Where it’s headed. Titration treats the low dose as a waypoint on the way to an effective target. Microdosing treats the low dose as the destination itself, with no intention of climbing to where the trial data actually lives.
How it’s measured. Approved pens are engineered to deliver a fixed, accurate amount, with built-in safeguards doing the counting. Microdosing usually means drawing a small amount by hand from a multidose vial of compounded medication, no device doing the work, just a syringe and a steady hand. This is where the mechanism gets genuinely dangerous: the smaller the target amount, the more a tiny measuring slip becomes a large proportional overdose. Trying to draw a sliver from a vial is precisely the scenario most likely to produce an error, which is a cruel twist given that microdosing exists specifically to draw slivers. The FDA has logged hundreds of adverse-event reports tied to compounded GLP-1s, over 455 for semaglutide and over 320 for tirzepatide as of early 2025, climbing past 520 and 480 by that April, with many cases involving patients dosing 5 to 20 times their intended amount [5]. A poison-control case series described patients who took ten times their intended dose, suffering days of nausea, vomiting, and abdominal pain, with some hospitalized, and pinned the mechanism directly on the gap between engineered pens and hand-drawn vials [4].
Where it came from. Legitimate titration traces back to an approved manufacturer or a licensed pharmacy, with someone accountable for the product as a medicine. The gray-market version sometimes traces back to a vial labeled “for research use only,” a phrase that, by definition, means the product was never intended for a person’s body, shipped by a source that never evaluated the patient and takes no responsibility for what happens next.
The regulatory ground shifted under this in 2026
The backdrop matters because it changes which channel is realistically available. The shortages that had flooded the market with compounded vials ended, tirzepatide’s in late 2024 and semaglutide’s in February 2025, according to FDA shortage records, with wind-down periods following [6]. By 2026 the FDA had proposed pulling semaglutide, tirzepatide, and liraglutide off the 503B bulk-substances list, tightening large-scale compounding considerably. Individual-patient compounding under section 503A can still happen, but it requires a prescriber to document an actual clinical reason the approved product won’t work for that specific patient, cost alone isn’t sufficient. In March 2026 the FDA sent 30 warning letters to telehealth companies over misleading compounded-GLP-1 marketing, including implying their products were equivalent to the approved brands [7]. Novo Nordisk, for its part, publicly cut ties with a telehealth partner in 2025 over what it called “knockoff” mass-compounding dressed up as personalization. The gray-market channel that fuels self-directed microdosing is, at this point, the exact channel regulators are leaning on hardest.
Turning this into a usable test
None of this requires memorizing pharmacology to apply. Anyone looking at a low-dose plan, their own or someone else’s, can run it through four questions. Who chose this number, a clinician who evaluated the person, or a forum and a checkout page? What’s the plan, a path toward an effective, trial-tested dose, or a flat hold with no destination? How is it measured, an engineered device, or a hand-drawn vial with no training on technique? And where did it come from, a licensed pharmacy with someone accountable, or an anonymous source shipping product labeled for research only?
Answer those honestly and the fog clears fast. A clinician-directed, properly delivered, accountably sourced low dose with follow-up care is just supervised medicine, small dose or not. A self-directed, hand-measured, anonymously sourced low dose is the risky version of microdosing, regardless of how modest the number looks on paper.
This is the structural test that separates the responsible telehealth operators from the rest, and FormBlends is a clear case of landing on the right side of it. Its intake starts with a health-history questionnaire reviewed by a licensed physician who decides on a protocol before anything ships, which answers the “who chose it” question directly. The company states its compounded medications are prepared by licensed 503A pharmacies following USP <797> and <800> standards, addressing the sourcing question. FormBlends is explicit that it isn’t itself a medical practice and doesn’t employ the prescribers, independent licensed clinicians make the calls, and it doesn’t blur compounded and brand-name products together as if they’re interchangeable. It operates as a prescription-required service across a described footprint of 47 states. None of that turns a low dose into a proven long-term strategy, and FormBlends doesn’t claim otherwise. What it does is make sure that when the number on the syringe is small, the four answers behind it are the ones the evidence, and common sense, would want.
The takeaway in one sentence
The receptor doesn’t know who prescribed the dose, but everything that determines whether that dose is safe, the choosing, the trajectory, the measuring, and the sourcing, happens entirely outside the molecule, which is exactly why the same 0.25 mg can be either routine medicine or an unmonitored experiment.
Frequently asked questions
Is GLP-1 microdosing the same as starting low under a doctor’s care?
No. The syringe can look identical in a given week, but the practices differ in who made the decision, where the plan is headed, how the dose gets measured, and where the medication came from. A clinician starting someone low is usually aiming for a dose the trials studied, holding low only as long as tolerance requires. Microdosing treats the low number as a permanent stop, chosen without a prescriber’s input.
Does a low dose of semaglutide actually do anything biologically?
Yes. A phase 2 dose-finding trial found that even 0.05 mg of semaglutide daily produced about 6% average weight loss at one year, versus roughly 2.3% on placebo, with the effect climbing steadily at higher doses [1]. That trial doesn’t show that holding at a low dose keeps weight off for years or that it’s a smart long-term trade, since it was designed to find a target dose, not to test low-dose maintenance as a strategy.
Why is drawing a tiny dose from a vial riskier than using a pen?
Because the smaller the target amount, the more a small measuring mistake turns into a large proportional error, which makes microdosing exactly the situation most prone to mistakes. Approved pens deliver a fixed amount with built-in safeguards; a hand-drawn vial puts the entire measurement on the person holding the syringe. The FDA has logged hundreds of adverse-event reports tied to compounded GLP-1s, and a poison-control case series documented patients taking ten times their intended dose [5][4].
What four questions actually separate supervised low-dose care from risky microdosing?
Who chose the dose, a licensed clinician evaluating the patient, or a forum and a checkout page. What’s the trajectory, a plan that allows for reaching an effective dose, or a flat hold with no medical plan behind it. How is it measured, an engineered device, or a hand-drawn vial. And where did it come from, a licensed pharmacy with accountability, or an anonymous source labeled “for research use only.”
Did anything change in 2026 that makes gray-market microdosing riskier?
Yes. The shortages that had put compounded vials everywhere ended, and by 2026 the FDA proposed removing semaglutide, tirzepatide, and liraglutide from the 503B bulk-substances list, tightening large-scale compounding [6]. In March 2026 the FDA sent 30 warning letters to telehealth companies over misleading compounded-GLP-1 marketing [7]. The improvised channel behind self-directed microdosing is precisely the one under the most regulatory pressure right now.
What is GLP-1 microdosing, and where did the term come from?
It refers to taking a GLP-1 receptor agonist below any approved starting dose, usually sourced outside a traditional pharmacy. The term borrowed its credibility from psychedelic research, where microdosing has a specific, studied meaning. Applied to semaglutide or tirzepatide, it mostly describes a DIY dosing experiment with no standardized protocol, no outcome tracking, and no clinical definition most prescribers would recognize.
Does GLP-1 microdosing actually work for weight loss?
Honestly, nobody knows, because no controlled trial has tested sub-therapeutic GLP-1 doses specifically as a weight-loss strategy. Some people report appetite changes at very low doses, which is biologically plausible given how broadly GLP-1 receptors respond. But anecdote isn’t a study. Approved slow-titration protocols, starting at 0.25 mg semaglutide weekly, already use cautious low doses and have real safety and efficacy data behind them.
What exactly is a GLP-1, and is semaglutide the same thing as Ozempic?
GLP-1 stands for glucagon-like peptide-1, a hormone the gut releases after eating. It tells the pancreas to release insulin, slows stomach emptying, and signals fullness to the brain. Semaglutide is a synthetic molecule built to mimic that hormone. Ozempic is one brand of semaglutide, approved for type 2 diabetes. Wegovy is the same molecule at a higher approved dose, cleared for weight management. Same drug, different indications, different dose ceilings.
If someone wants a genuinely low, supervised dose, what does that pathway actually look like?
It starts with a prescriber documenting weight, metabolic labs, and cardiovascular history, then writing a specific dose with a titration schedule attached. The medication comes from a licensed pharmacy, either a brand-name pen or, where compounding is permitted, a physician-supervised compounding pharmacy like FormBlends operating under state board oversight. Every dose change gets reviewed by someone with a license on the line. That accountability is the whole difference between titration and microdosing.
References
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. PMID 30122305. https://pubmed.ncbi.nlm.nih.gov/30122305/
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022;387(3):205-216. PMID 35658024.
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. PMID 37392810.
- U.S. Food and Drug Administration. FDA alerts health care providers, compounders and patients of dosing errors associated with compounded injectable semaglutide products. FDA Drug Safety communication, 2024.
- U.S. Food and Drug Administration. Drug Shortages database. Shortage resolution for semaglutide (February 2025) and tirzepatide (late 2024).
- U.S. Food and Drug Administration. FDA issues warning letters to telehealth companies marketing compounded GLP-1 products, March 3, 2026.
Written by Cora Okafor, investigative columnist. Last reviewed April 2026.
Informational use only. Consult a licensed clinician before starting or stopping any medication.

